⸺Scoliosis⸺
Scoliosis is the general term for a deformation of the spine and is derived from the Greek word [scolios] for “crooked”. It can occur in all sections of the spine from the neck to the lumbar vertebrae, sometimes in several positions at the same time.
We can distinguish between idiopathic and secondary scoliosis. Secondary scoliosis is rarer and often a result of malformations, systemic diseases, nerve or muscle diseases. Eighty to 90 per cent of scoliosis cases are called idiopathic scoliosis, where the cause is not fully understood. However, hormonal, neuronal and muscular disorders are thought to be the triggers. The tendency to scoliosis seems to be inherited, as the condition runs in families.

Idiopathic scoliosis
If idiopathic scoliosis occurs before the age of three, it is called infantile scoliosis, between the ages of four and ten it is called juvenile scoliosis and from the age of 11 it is called adolescent scoliosis. So-called adult scoliosis is becoming increasingly common in adults.
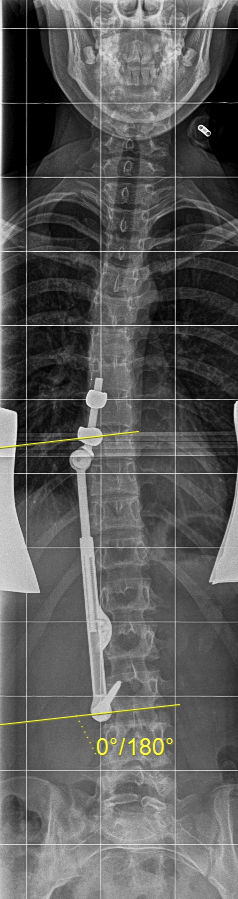
In the UK, three to five per cent of the population is affected by the condition. Scoliosis is classified according to the Cobb angle, which indicates the degree of curvature of the spine, and is therefore a measure of the severity of scoliosis. This angle can be measured in an X-ray. By definition, scoliosis is only considered to be at a Cobb angle of 10°. Girls are six times more likely to develop the disease than boys, and scoliosis above a Cobb Angle of 30° affects ten times more girls than boys.
If scoliosis is not treated, the deformation of the spine will usually continue to increase.
This can lead to movement restrictions, stiffening and wear and tear in the affected or adjacent spinal sections. Advanced scoliosis can be identified, for example, by an appearance of a rib hump or rib valley, an asymmetric shape of the neck muscl
Conservative treatment
After the first diagnosis of scoliosis in the child and a scoliosis degree up to 20° Cobb angle, a conservative treatment plan is initially developed:
This includes educating parents and young patients, physiotherapy, possibly adjusting inserts for different leg lengths, and regular monitoring by the attending physician. If the degree of scoliosis exceeds 20°Cobb angle and other risk factors such as the child's age, maturity and rapid progression of scoliosis, corset therapy is usually recommended. The corset is a so-called growth-controlling measure.
It is intended to at least partially correct the scoliosis and maintain this reduced curvature until the end of growth. The corset is made from thermoplastic plastic and its shape exerts pressure against the outside of the curvature. To be effective, it must be worn day and night. The aim is to avoid surgery or, in very young patients, at least, delay. When used correctly and with good cooperation from the patient and family, the effect of the corset therapy is scientifically proven. The basis for successful conservative therapy is the adaptation of the first corset by an experienced corset maker, accompanying physiotherapy and learning of its own exercises.





Surgical therapy
If the scoliosis progresses rapidly, surgery may be necessary. The aim is to correct the scoliosis, restore good balance and, last but not least, improve optics.
During surgery, significant corrections of scoliosis can be achieved by screws inserted into the spine in conjunction with rods. The more pronounced the scoliosis becomes and the stiffer the spine, the greater the surgical effort of a scoliosis correction.
Some idiopathic scoliosis deteriorates rapidly during the growth phase and especially during puberty. In this situation, too long, untreated course can lead to severe curvatures at the end of growth, which often require costly surgical correction. In addition to a good corset therapy, so-called growth-directed surgical correction procedures are also used successfully. These include Apifix and VBT (Vertebral Body Tethering).
In recent years, the ApiFix procedure has been increasingly used as an alternative to classic stiffening surgery for patients whose spine is still sufficiently flexible and the curvature is not too advanced. The ApiFix system is fixed at three points of the spine and can then be stretched according to the ratchet principle so that the spine is erected. This method has many advantages: the spine remains mobile and the operation is less time-consuming. It takes about an hour, there is only a small blood loss and after three to four days the patient can go home.
The implant is removed after completion of growth or at the latest 3-4 years after implantation.
Adult Scoliosis
If patients are older than 30, they are referred to as adult scoliosis. Most often, degenerative processes, hormonal changes in old age, especially in women, and reduced bone density such as osteoporosis are causes for the development of scoliosis in old age. Typical symptoms can include local back pain and radiating pain in the legs, functional limitations and movement deficits.
Conservative treatment
The first line of treatment for adult scoliosis is always physiotherapy and physical interventions supported by pain medication. Targeted injections, general muscle building and weight reduction also relieve discomfort for many sufferers.
Surgical therapy
In case of severe pain or neurological failure, surgery is usually required. Modern techniques and surgical procedures make it possible to safely treat even elderly patients.
